- Research article
- Open access
- Published:
Using total quality management approach to improve patient safety by preventing medication error incidences**
BMC Health Services Research volume 17, Article number: 621 (2017)
Abstract
Background
Whereas one of the predominant causes of medication errors is a drug administration error, a previous study related to our investigations and reviews estimated that the incidences of medication errors constituted 6.7 out of 100 administrated medication doses. Therefore, we aimed by using six sigma approach to propose a way that reduces these errors to become less than 1 out of 100 administrated medication doses by improving healthcare professional education and clearer handwritten prescriptions.
Methods
The study was held in a General Government Hospital. First, we systematically studied the current medication use process. Second, we used six sigma approach by utilizing the five-step DMAIC process (Define, Measure, Analyze, Implement, Control) to find out the real reasons behind such errors. This was to figure out a useful solution to avoid medication error incidences in daily healthcare professional practice. Data sheet was used in Data tool and Pareto diagrams were used in Analyzing tool.
Results
In our investigation, we reached out the real cause behind administrated medication errors. As Pareto diagrams used in our study showed that the fault percentage in administrated phase was 24.8%, while the percentage of errors related to prescribing phase was 42.8%, 1.7 folds. This means that the mistakes in prescribing phase, especially because of the poor handwritten prescriptions whose percentage in this phase was 17.6%, are responsible for the consequent) mistakes in this treatment process later on. Therefore, we proposed in this study an effective low cost strategy based on the behavior of healthcare workers as Guideline Recommendations to be followed by the physicians. This method can be a prior caution to decrease errors in prescribing phase which may lead to decrease the administrated medication error incidences to less than 1%.
Conclusion
This improvement way of behavior can be efficient to improve hand written prescriptions and decrease the consequent errors related to administrated medication doses to less than the global standard; as a result, it enhances patient safety. However, we hope other studies will be made later in hospitals to practically evaluate how much effective our proposed systematic strategy really is in comparison with other suggested remedies in this field.
Background
Problem description
Medication errors are the most common type of medical errors in healthcare sectors. They may cause or lead to inappropriate medication use or patient harm [1]. 6–7% of hospital admissions are due to medication errors [2].
Available knowledge
Medication error is a harmful event that may occur in different stages of patient treatment process. Hence, which step caused the problem cannot be well determined. However, medication errors can generally be classified either according to the stage of their occurrence (i.e. prescribing, drug administering, dispensing or error monitoring) or according to their damage intensity [3].
World Health Organization summarized in its recent report related to medication errors the key factors that may lead to the occurrence of these errors. These factors can be attributed to health care professionals, patients, work environment, medicines, tasks, computerized information systems, or primary-secondary care interface issues [3].
Different approaches were proposed to solve this problem. One of them is restoring to automated data systems, medication reviews and reconciliation, educating health care workers, and identifying Multicomponent interventions [4,5,6,7,8].
Rational and specific aims
Total Quality Management (TQM), is a methodology of management for continuously improving the quality of products and processes to meet or exceed customer expectations [1], and; on the other hand, Six Sigma is a business management strategy which seeks to improve the quality of process outputs. This business management depends on using a set of tools which are known as DMAIC (Define, Measure, Analyze, Improve, and Control). Therefore, Integrating Six Sigma with TQM program improves the process through detailed data analysis, and it makes TQM efforts more successful [9]. In other words, the achievement of six sigma methodology applied in this research paper, integrated with TQM, was a trial to work on health care professional educating to prevent medication errors occurring in healthcare sectors. We aimed to reduce the medication error incidence to less than the global standards indication; 1 out of 100 administrated medication doses, within a period of 13 weeks with no high expenditure.
Methods
A medication error is any harmful event that may cause or lead to an inappropriate medication use or patient harm whether such an error comes from the health care professional, the patient, or the consumer. These errors are typically considered to be related to administration of a medication. In fact, they may also include errors in ordering or delivering the medications [10].
We used the following definitions of medication errors according to the step of their occurrence:
Prescribing errors
They occur as a result of a prescribing decision or prescription writing process [10]. It includes mistakes made by the physician when ordering a medication; incorrect drug selection, route, the frequent of administration,, dosage form, instructions for use of a drug product, wrong drug, drug to which patient is allergic, Drug-Drug Interactions (DDIs), bad Controlled Drug Substances (CDS), not following good CDS, and wrong patient errors [11].
Administration errors
Such errors usually occur when deviating from the physician’s order according to what is written in the patient’s chart [12]. They errors include unlicensed drug, over dose, wrong dose, missing dose, wrong form of administration, wrong technique, wrong time [13].
Dispensing errors
The deviations from the physician’s order, made by the pharmacy staff when distributing the medications to the nursing team or to the patients in an ambulatory setting [14]. The dispensing process is an integral part of the quality of medicine usage that forms together with patient counseling the core professional activities of a pharmacist. The process of dispensing and counseling is composed of a sequence of steps. If any of these steps has been interrupted or completed incorrectly, this could result in poor quality outcomes for the patient. This type of errors generally refers to errors in the dispensing process (wrong drug, wrong dose strength, incorrectly labeled directions, or drug dispensed to wrong patient). These errors cannot be detected or corrected prior to the patient leaving the pharmacy. This may lead; as a consequence, to less effective outcomes of treatment for the patient [15].
Monitoring errors
They are the failure to review a prescribed therapeutic plan for appropriateness and detection of problems, or weakness to use appropriate clinical or laboratory data for adequate assessment of patient response to prescribed therapy [16].
Interventions, measures and analysis
This project was conducted at a general governmental hospital. The number of beds was 93 beds, and the number of physicians was 137 physicians, and the number of nurses was 318 nurses. We systematically studied the process of medication application by the health care professionals in this hospital. Then, we introduced six sigma in our health care setup for the provision of the patient’s safety. Six Sigma’s approach of problem (Definition, measurement, and statistical analysis, improvement, and control plans) was involved in our study. The six sigma quality improvement team used the five-step DMAIC process for every project [17].
In other words, we formulated theories by brainstorming to figure out the real causes of medication errors after studying the applied treatment process. For that, Medication Error Causes- Data Sheet was used to determine the real cause behind each type of medication errors defined above and its percentage. This was based on nurses’ answers. Data-analysis tool was Pareto diagram.
Table 1 defines each phase of the DMAIC process (Define, Measure, Analyze, Implement, Control).
Results and discussion
Definition phase
Medication errors are a global issue that causes harm and even death. They are very costly and adversely influence patients’ safety, nurses and organizations.
A previous study in our pilot investigations and reviews estimated that the incidence of medication errors was 6.7 out of 100 administrated medication doses, while the global standards indicated that the incidence of medication errors should not exceed 1 out of 100 administrated medication doses.
Our objective is to reduce the medication error incidence to less than 1 out of 100 administrated medication doses, within a period of 13 weeks with no high expenditure.
Measurement phase
SIPOC
Suppliers (Patient, Physician, Nurse, Pharmacist, Pharmacy), Inputs (Patient, Prescription, drugs), Process (Prescribing, Dispensing, Administrating, Monitoring), Outputs (Selected Drugs), Customers (Patient, Physician, Nurse, Pharmacist). Figure 1 shows SIPOC for medication process.

SIPOC for Medication process (Suppliers, Inputs, Process, Outputs, Customers)
Voice of the customer
It includes four steps as shown in Table 2. Table 3 shows the customer feedback, Critical Customer Requirements (CCRs), Critical to Quality (CTQs), and Targets.
Analyzing symptoms
(Incidence of medication errors)
Operational definition
See Methods section of this research paper. We would measure the Incidence of medication error by measuring the following rates through observation methods of process or self-reporting:
-
1.
Wrong prescription error repetition rate
-
2.
Wrong drug administration errors rate
-
3.
Wrong dose administration errors rate
-
4.
Wrong route administration errors rate
-
5.
Wrong administration errors repetition rate
Operational definitions can be seen in Table 4.
Define the boundaries
Table 5 presents the boundaries of the process. Figure 2 shows the high level flow diagram in the medications use process, Fig. 3 shows detailed flow diagram of medication use process, and Fig. 4 shows cause effects diagrams.

High level flow diagram in the medication use process

Detailed flow diagram medication use process

Cause-effect diagrams
Analysis phase
Formulate theories through brainstorming
This was used to determine the full range of possible causes. Table 6 shows the formulation of theories through brainstorming.
Cause-effect diagrams
We categorized the causes according to process steps
-
1.
Prescribing
-
2.
Dispensing
-
3.
Administrating
-
4.
Monitoring
Data collection
The data which we need are not available; we don’t have reports about the medications error and no registration system of any related data, so the method of data collection we selected was medication error causes- data sheet which must be filled by nurses. Table 7 shows the Medication Error Causes- Data Sheet.
Whereas nurses play multifarious roles in medication use process, they are the cornerstone in the medication use process; nurses involve in all process steps and understand the process. They receive orders from physicians, receive drugs from pharmacy, administrate the drugs to the patient and finally monitor the response.
Therefore, Data sheet was set to investigate “Why Medication Errors occur”, and every nurse should select three causes of the sheet. One hundred and six sheets were filled and analyzed. The following table; Table 8, shows the total score of each cause of medication error.
Data-analysis
Data-analysis tool is Pareto diagram, to focus on the vital few. The goal of the Pareto is to separate the causes of problems into the vital few and the useful many. Pareto diagram was used to present the results (Tables 9, 10, 11 and 12 & Figs. 5, 6, 7 and 8) reveal the contributors, magnitude and cumulative percent.

Pareto diagram- causes of medication error (N = 318) * \ Caption: Results from Table 9 (Pareto table --causes of medication error) were presented as Pareto Diagram

Pareto diagram -cause of error during phases of medication process (N = 318)

Pareto diagram- causes of medication error related prescribing phase (N = 318)

Pareto diagram- causes of medication error related prescribing phase after groping the causes related to prescribing behavior of physicians (poor handwriting orders, unapproved abbreviations, metric & apothecary systems and unnecessary decimal points) (N = 318)
Causes of medication error
Pareto diagram does not produce a clear picture of the vital few because each of the categories is nearly equal in the score. The data indicate no clear distinction among the categories.
All the bars on a Pareto diagram roughly have the same height, and it takes more than half of the categories to account for more than 60% of the quality effect.
Data were stratified by process steps, then we selected the first phase which had the higher scores and then we grouped the causes resulted from (poor handwriting orders, unapproved abbreviations, metric & apothecary systems and unnecessary decimal points).
Identify root causes
Root Causes are causes resulted from traditional prescribing behavior of physicians:
-
1.
Poor handwriting orders
-
Ambiguous
-
Illegible
-
Incomplete
-
2.
Unapproved abbreviations
-
3.
Metric systems
-
4.
Unnecessary decimal points
The proposed root causes are controllable because they are related to one factor of the process applied by the physicians who prescribe the drugs (prescribing behavior or practice).
Improvement phase
Evaluate the alternatives
Formulate remedies through brainstorming
-
1.
Automation and technology: In hospitals, this can be by the presence of computerized medication records such as electronic prescribing, bar coding, and automated drug-dispensing systems.
-
2.
Demand on the nursing staff: Strategies to promote greater accuracy in drug administration account for increased demand on licensed nurses.
-
3.
Education & training of nursing staff: Many hospitals spend a lot of money on high-technology equipment, but not enough on educating the nurses. This remedy is very important as nurses are who administrate the medications in most cases.
-
4.
Standardized general principle & practices of medication administration through six rights: Nurses attempt to ensure that the Right drug is given in the Right dose at the Right time via the Right route to the Right patient and with right documentation
-
5.
Double check system: This is by Double-check for every medication every time by a second person.
-
6.
Organization’s Policies & Procedures: They are less expensive strategies that can be applied in the hospitals to reduce medication administration errors.
-
7.
Suitable work environment: Suitable work environments should be available for the safe preparation of drugs
-
8.
Reporting about the incidence of medication error: Reporting about the drug administration errors via incidence report is considered a professional and ethical responsibility of all health care providers
-
9.
No punitive actions: Managers are responsible for ensuring that nurses and other providers are punished for the medication errors they make. Hence, error reporting is encouraged.
-
10.
Empowerment: Nurses’ participation in problem solving is the best way to derive strategies that will be effective and feasible. Nurses have to be involved from their unit level through the hospital policy level in decisions affecting medication administration accuracy
-
11.
Medication Safety Committee: Every hospital should have a medication safety committee
For evolution purpose we have organized the remedies in two main strategies that include the following:
-
Strategy (I): Improvement of handwritten prescriptions.
-
Strategy (II): Eliminating all handwritten prescriptions by Implementing computerized order entry
Evaluate the alternatives
Strategies to Improve Medication Safety:
-
1)
Improve handwritten prescriptions by Support efforts to increase prescription legibility and Developing & disseminating guideline to improve handwritten prescriptions
- Use of standard prescription preparation practices in the education and continuous education of physicians.
- Standardize prescription writing way and its rules, include the purpose(guideline)
- Establish and use the standard terminology elements.
- Encourage physicians to avoid using drug name abbreviations on all prescriptions and drug orders.
- Ask the physicians to add a notation of purpose (not necessarily diagnosis) on all prescriptions.
- Ask the physicians to add a notation on the prescription for a child patient, and to mention the exact age of the child who is less than 14 years of age.
-
2)
Eliminate all handwritten prescriptions.
- Use electronic entry, hand-held computer, or other similar technology
- Use automated drug-ordering systems.
- Implement physician order entry.
- Ask for Physicians’ direct computer entry of prescriptions
- Physician entry of prescriptions on a computer reduces transcription errors and shows potentially problematic prescriptions. For instance, it shows an improper dose being prescribed or a drug that might interact with another medication taken by the patient.
- Automated hospital dispensing systems notify nurses when a drug is to be administered. The systems also record what has been given and when as well as reduce the delays in giving patients their medications and decrease other administration errors.
- Barcoding hospital medications: Machine-readable labels can facilitate matching patients with their prescribed medications and documenting drug dispensing and administration.
- Computerized medication errors monitoring: Computer programs are designed to show potential medication errors, using data from electronic patient medical records (e.g., orders for known antidotes or specific laboratory test abnormalities).
Evaluation criteria: The two aforementioned strategies were evaluated according to the following criteria:
- Total Cost | - Implementation Duration |
- Impact on the Problem | - Uncertainty about Effectiveness |
- Benefit/Cost Relationship | - Health & Safety |
- Cultural Impact/Resistance to Change | - Environment |
Each strategy was given a score from H to L through M where (H = High Desirability and M = Medium Desirability, while L = Low Desirability). Table 13 shows Remedy Selection Matrix and according to this matrix the selected strategy was Improvement of handwritten prescriptions by supporting traditional process of prescribing.
-
The planning matrix, Fig. 9, shows the process that will be conducted to implement the selected remedial strategy.
Fig. 9 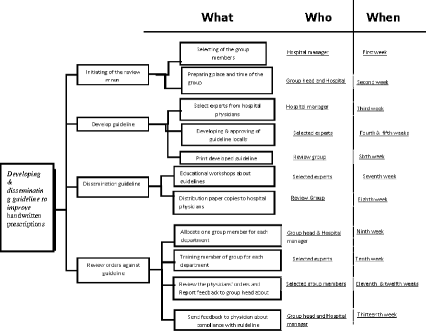
Planning matrix

Planning step included:
- Establishing review group (committee)
- Developing guideline for prescribing
- Disseminating guideline to all physicians through educational workshops
- Training members of review group to review prescribing orders in accordance with the guideline recommendations Design remedy: The required resources:
-
People: a review group to be consisted of a qualified physician as head of the group, a nurse assistant to the physician, five secretaries for hospital units and departments, and one clerk. Unit secretary in each department should be trained to review drug orders (prescriptions) in accordance with the guideline recommendations, and report to group administrators.
-
Money: Costs of development and dissemination of the guidelines, training of medical secretary
-
Duration: nine weeks
-
Materials: Place of review group and material needed for print the guideline and circulation of the guideline to all the physicians in the hospital
Design for culture
- Sources of barriers and aid.- Countermeasures needed to overcome barriers.
Barriers are: Shortage in nurses, Physician acceptance, Physician time.
Aids are: Involvement & commitment of Top Management
Counter measures include Training of medical secretary, Participating in developing the guideline, Educational workshops about guidelines.
The design for culture can be seen in Fig. 10

The design of culture
Prove effectiveness: (pilot test, implement plan)
- Pilot test
The strategy was implemented on the outpatients on a limited scale
- Implement Plan
-
1)
Educational workshops for physicians about Guideline Recommendations
-
2)
Training of unit secretaries on their responsibilities which include review prescribing orders in accordance with the Guideline Recommendations (Table 14).
Table 14 Guideline recommendations to improve handwritten prescriptions
Control phase
Preservation the remedy
Unit secretary reviews prescriptions in accordance with the guideline, if order is: ambiguous, illegible or incomplete or includes unapproved abbreviations. Then the unit secretary resends the prescription to physician to correct it. Figure 11 shows the feedback loop, and Fig. 12 shows Detailed flow diagram new medication use process.

Feedback loop

Detailed flow diagram new medication use process
Audit the controllers
○ The Head of review group should aggregate the rate of incidence of medication errors and should report the percentage to the hospital manager regularly.
○ The Head of review group should count the percentage of compliance of the physicians with the guideline and should send to the hospital manager regular reports about the level of compliance of the physicians. Then, the hospital manager will handle this issue with the physicians in his regular meetings with the medical staff.
○ Each prescription should be reviewed in dependence on the Review Sheet in accordance with the Guideline Recommendations (1), Additional file 1
○ The data that were included in the Review Sheet in accordance with the Guideline Recommendations should be aggregated in Daily Review Sheet (2), Additional file 2
○ For each physician the level of compliance with the guideline should be assessed using the formulas of Indicators for Guideline (3), Table 15
○ Results of computing the indicators should be compared with the standards. Each division should report to the manager to take the appropriate corrective actions.
Conclusions
Since medication errors are a global threat for healthcare workers’ and patients’ safety we tried in our study to apply Six Sigma set of steps (DMAIC) integrated into TQM tools to recommend a new technique to prevent medication error incidences in healthcare sections. First, we defined the medication errors and determined their problems to set the objective of this study which is reducing the incidence of administrated medication doses to meet the global standards without any extra cost. Then, we moved to the “measure” phase of six sigma approach. We were able to determine SIPOC for medication process, listen to The Voice Of The Customer, and to define the operation with its boundaries. In analyzing step, we formulated theories through brainstorming to consider the full range of possible causes of medication error incidences by data collection using Medication Error Causes- Data Sheet. Then, we analyzed the collected data using Pareto Diagrams to determine the Vital Few. In this step, we found that Prescribing Error Incidences occur in 42.8% after which come Administrating Errors, monitoring Errors and Dispensing Errors, with 24.8%,18.2%,14.2% respectively. In prescribing error incidences the poor handwriting orders had a higher score than other sub-causes. Therefore, we compared between two strategies for this sub-causes using Remedy Selection Matrix in the “Improve” phase of six sigma steps. The two main improvement strategies were either to improve the prescription hand writing or to eliminate them by automation. According to this matrix, the selected choice was to support handwritten prescriptions by suggestion of assistant sheets; Guideline Recommendations to Improve Handwritten Prescriptions to be used by the physicians working in the Hospital. To prevent the remedy, we kept the feedback loops as short as possible. A number of sheets were also suggested in the control step to audit the controllers. These sheets are Review Sheets in accordance with the Guideline Recommendation, Daily Review Sheets, and Indicators for Guideline. Finally, we hope that this proposed strategy for improving mediation use will be applied by other healthcare researches, to know how much effective it is and how much it does improve the medication use process which ensures that each patient will have his or her own suitable drugs away from medication errors and the adverse effect incidences.
Abbreviations
- CCRs:
-
Critical Customer Requirements
- CDS:
-
Controlled Drug Substances
- CTQs:
-
Critical to Quality
- DDIs:
-
Drug-Drug Interactions
- DMAIC:
-
Define, Measure, Analyze, Implement, Control
- TQM:
-
Total Quality Management
References
Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, et al. The nature of adverse events in hospitalized patients. Results of the Harvard medical practice study II. N Engl J Med. 1999;324:377–84.
Alexopoulou A, Dourakis SP, Mantzoukis D, Pitsariotis T, Kandyli A, Deutsch M, et al. Adverse drug reactions as a cause of hospital admissions: a 6-month experience in a single center in Greece. Eur J Intern Med. 2008;19:505–10.
Medication Errors. Technical series on safer primary care. Geneva: World Health Organization; 2016. Licence: CC BY-NC-SA 3.0 IGO
Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172:1057–69.
Radley DC, Wasserman MR, Olsho LE, Shoemaker SJ, Spranca MD, Bradshaw B. Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. J Am Med Inform Assoc. 2013;3:470–6.
Roque F, Herdeiro MT, Soares S, Teixeira Rodrigues A, Breitenfeld L, et al. Educational interventions to improve prescription and dispensing of antibiotics: a systematic review. BMC Public Health. 2014;14:1276.
Pedersen JS, Brereton L, Newbould J, Nolte E. The puzzle of changing relationships. Does changing relationships between healthcare service users and providers improve the quality of care. London: The Health Foundation; 2013.
Holloway KA, Ivanovska V, Wagner AK, Vialle-Valentin C, Ross-Degnan D. Have we improved use of medicines in developing and transitional countries and do we know how to? Two decades of evidence. Tropical Med Int Health. 2013;18:656–64.
Aized T. Total quality management and six sigma. 1st ed. Croatia: InTech; 2012.
Dean B. What is a prescribing error? Qual Health Care. 2000;9:232–7.
Velo G, Minuz P. Medication errors: prescribing faults and prescription errors. Br J Clin Pharmacol. 2009;67(6):624–8.
Keers R; Williams S; Cooke J; • Ashcroft D, Causes of medication administration errors in hospitals: a systematic review of quantitative and qualitative evidence, Drug Saf (2013) 36:1045–1067.
Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Arch Intern Med. 2002;162:1897–903.
Anacleto TA, Perini E, Rosa MB, Cesar CC. Medication errors and drug-dispensing systems in a hospital pharmacy. Clinics. 2005;60:325–32.
Ka C, Bouvy M, De Smet P. Medication errors: the importance of safe dispensing. Br J Clin Pharmacol. 2009;67(6):676–80.
Peterson GM, Wu MS, Bergin JK. Pharmacists’ attitudes towards dispensing errors: their causes and prevention. J Clin Pharm Ther. 1999;24:57–71.
Simmons-Tau D, Cenek P, Counterman J, Hockenbury D, Litmiller L. Reducing VAP with 6 sigma. N-urs Manag. 2004;35:41–5.
Acknowledgements
- Damascus National University.
- Al- Andalus Private University for Medical Sciences.
- The general governmental hospital where the study was conducted.
- Dr. Adnan Badour for his performing the statistical analysis
- Wardeh office for Translating representative with Mr. Nabeel Wardeh: Arabic- English sword translator.
Funding
It was provided by Government Hospital.
Availability of data and supporting materials
Data are contained in the text.
Author information
Authors and Affiliations
Contributions
FY designed the study, coordinated and helped to draft the manuscript. NY participated in the study and helped in ESL issues. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not applicable in this section.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1: Table S1.
Review Sheet against Guideline Recommendations (1) (N= 318). (DOCX 14 kb)
Additional file 2: Table S2.
Daily Review Sheet (2). (DOCX 13 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yousef, N., Yousef, F. Using total quality management approach to improve patient safety by preventing medication error incidences** . BMC Health Serv Res 17, 621 (2017). https://doi.org/10.1186/s12913-017-2531-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-017-2531-6