- Research
- Open access
- Published:
Improved hypertension control at six months using an adapted WHO HEARTS-based implementation strategy at a large urban HIV clinic in Uganda
BMC Health Services Research volume 22, Article number: 699 (2022)
Abstract
Objectives
To adapt a World Health Organization HEARTS-based implementation strategy for hypertension (HTN) control at a large urban HIV clinic in Uganda and determine six-month HTN and HIV outcomes among a cohort of adult persons living with HIV (PLHIV).
Methods
Our implementation strategy included six elements: health education, medication adherence, and lifestyle counseling; routine HTN screening; task shifting of HTN treatment; evidence-based HTN treatment protocol; consistent supply of HTN medicines free to patients; and inclusion of HTN-specific monitoring and evaluation tools. We conducted a pre-post study from October 2019 to March 2020 to determine the effect of this strategy on HTN and HIV outcomes at baseline and six months. Our cohort comprised adult PLHIV diagnosed with HTN who made at least one clinic visit within two months prior to study onset.
Findings
We enrolled 1,015 hypertensive PLHIV. The mean age was 50.1 ± 9.5 years and 62.6% were female. HTN outcomes improved between baseline and six months: mean systolic BP (154.3 ± 20.0 to 132.3 ± 13.8 mmHg, p < 0.001); mean diastolic BP (97.7 ± 13.1 to 85.3 ± 9.5 mmHg, p < 0.001) and proportion of patients with controlled HTN (9.3% to 74.1%, p < 0.001). The HTN care cascade also improved: treatment initiation (13.4% to 100%), retention in care (16.2% to 98.5%), monitoring (16.2% to 98.5%), and BP control among those initiated on HTN treatment (2.2% to 75.2%). HIV cascade steps remained high (> 95% at baseline and six months) and viral suppression was unchanged (98.7% to 99.2%, p = 0.712). Taking ART for more than two years and HIV viral suppression were independent predictors of HTN control at six months.
Conclusions
A HEARTS-based implementation strategy at a large, urban HIV center facilitates integration of HTN and HIV care and improves HTN outcomes while sustaining HIV control. Further implementation research is needed to study HTN/HIV integration in varied clinical settings among diverse populations.
Introduction
Background
Across low- and middle-income countries (LMIC), integrating the screening and treatment of hypertension (HTN) into existing HIV clinical care is widely recommended [1,2,3,4,5], yet its implementation remains suboptimal [6,7,8]. Integrated HTN/HIV care involves provision of both services for HTN and HIV in synchronized visits to the same clinic. This approach is more patient-centered than disease-specific or “vertical” programs and minimizes duplication and fragmentation of services, thus increasing efficiency [9]. Since HTN contributes the greatest population attributable risk for cardiovascular disease (CVD) among persons living with HIV (PLHIV) [10, 11], it is of great priority in efforts to integrate non-communicable diseases (NCDs) care with that of chronic HIV [4, 9]. There is an urgent need therefore to leverage the HIV infrastructure to provide contextually appropriate integrated HTN/HIV services in LMICs for dual control [12].
The World Health Organization (WHO) HEARTS technical packages for HTN management provide guidelines for HTN care on: healthy lifestyle, evidence-based protocols, access to HTN medicines, CVD risk assessment, task shifting and monitoring and evaluation [13,14,15,16,17]. Six-month control of blood pressure among people treated for HTN is a HEARTS Core Indicator [18]. The HEARTS tools are useful in the implementation of high-quality public health HTN management in LMIC settings. Though promising in improving HTN control among the general population, the effectiveness of WHO HEARTS in facilitating the integration of HTN care in the HIV clinical setting has not been studied [19, 20].
We recently conducted a mixed methods study at a large, urban HIV clinic (hereafter referred to as “Mulago ISS”) in Uganda which had achieved all the three UNAIDS 90–90-90 goals of initiating ART for PLHIV, retention in care, and viral suppression [21, 22]. In this clinic, there is a high prevalence of HTN (24.3%) among adult PLHIV. However, only one percent of these patients had been initiated on HTN treatment, 15% of those were retained in care, and, subsequently HTN control was achieved among only five percent [21]. We identified the barriers and facilitators of integrating HTN management into HIV care using qualitative methods, guided by the Capability, Opportunity, Motivation and Behavior (COM-B) model [21, 23, 24], which specifies that changing any behavior requires changing capability, opportunity and/or motivation to perform the desired behavior [23, 24]. Despite great interest in integrated HTN/HIV care from patients and providers as well as optimal patient adherence to available antiretroviral treatment (ART), the following were key barriers: suboptimal provider knowledge and skills for HTN care, lack of HTN treatment protocols, limited access to HTN medications and inadequate systems for monitoring and evaluation of HTN care [21].
Building upon these identified barriers, we undertook a systematic process to develop a HEARTS-based implementation strategy for HTN/HIV integration targeting both healthcare providers and patients [13]. This process involved using the Behavior Change Wheel (BCW) which is an intervention development framework that provides a comprehensive model of behavior change. It uses the COM-B model to understand behavior [13,14,15,16,17]. We mapped the barriers of HTN/HIV integration identified in our previous study onto the COM-B domains. The BCW framework was used to identify intervention functions to address barriers within each COM-B domain and to identify evidence-based behavior change techniques to carry out the intervention functions [23, 24]. We then adapted components of the HEARTS technical packages for cardiovascular control. Herein, we describe the baseline and six-month clinical outcomes of HTN and HIV among a prospective cohort of patients with both conditions who were provided integrated care at Uganda’s largest HIV clinic.
Methods
Study design
This was a pre-post study conducted between October 2019 and March 2020 to determine HTN and HIV treatment outcomes at baseline and six months after introducing a HEARTS-based implementation strategy for HTN/HIV integration at Mulago ISS.
Study setting
We conducted the study at Mulago ISS, a large HIV clinic in Kampala, Uganda that provides comprehensive HIV services to over 16,500 PLHIV. The clinic is located within the Mulago National Referral and Teaching Hospital Complex and is owned and operated by the Makerere University Joint AIDS Program (MJAP). HIV clinical services at Mulago ISS include HIV testing and counseling and provision of ART. All available HIV medicines and services at the clinic are provided at no cost to the patients.
In line with the Uganda National Guidelines for HIV care [25, 26], PLHIV at Mulago ISS are routinely screened for HTN. Prior to study commencement, the clinic had already achieved universal screening for HTN among all PLHIV during each clinic visit and had surpassed the 95% target of initiating ART among PLHIV. However, the clinic had no stock of HTN medications. Identified hypertensive PLHIV were given prescriptions to buy HTN medications from commercial pharmacies away from the HIV clinic. MJAP uses an electric medical records (EMR) system to facilitate clinical data capture and documentation.
This study was funded by Resolve to Save Lives, through its Learning, Implementation, Networking, Knowledge and Support (LINKS) program.
Developing the HEARTS-based implementation strategy for integrated HTN/HIV care
The implementation strategy, guided by the BCW, was developed through a series of four stakeholder meetings. Sixteen participants were purposively selected for these meetings, including two nurses, one pharmacist, one pharmacy technician, one laboratory technician, one clinic administrator, two social scientists and two monitoring and evaluation officers from the study site. Other participants included two HIV physicians, two cardiologists, and two Ministry of Health (MoH) NCD policy experts.
In the first two meetings, two investigators with expertise in implementation science (MM and RK) oriented meeting participants to the BCW framework, the nominal group technique for brainstorming [27], and the Affordability, Practicality, Effectiveness, Acceptability, Side effects, Equity (APEASE) criteria [28], for prioritizing implementation strategies.
Through brainstoming, meeting partcipants first identified intervention functions to address barriers to integrating HTN and HIV care. The following intervention functions were identified: education, training, enablement, persuasion, modeling, and environmental restructuring (Table 1). Using a scoring system of 1–6, the meeting participants applied the APEASE criteria to each intervention function to assess its appropriateness to integrated HTN/HIV treatment in Uganda [29]. After identifying the intervention functions, the team used the behavior change technique (BCT) taxonomy of the BCW to identify BCTs that best matched the selected intervention functions. BCTs are the active ingredients of an implementation strategy (Table 1) [30]. The team then brainstormed on the modes of delivery for the multi-component implementation strategy by adapting HEARTS components (Table 1). To determine local relevance, feasibility, and acceptability of the proposed implementation strategy, the last two stakeholder meetings reviewed the proposed modes of delivery to further refine the strategy. They achieved consensus on the relative importance and feasibility of each strategy thus contextualizing them to Ugandan HIV clinics. The multicomponent implementation strategy for integrated HTN/HIV care is described below and summarized in Table 1.
The strategy includes six major components:
-
1.
Health education, medication adherence, and lifestyle counseling
The HTN/HIV care protocol provided guidance to healthcare providers on health and lifestyle education for HTN. Health education to patients was provided by nurses and PLHIV peer educators and focused on possible side effects of medicines and their management as well as the need for and implementation of physical exercise, healthy diet, salt reduction, weight reduction, and smoking cessation. Nurses and dispensers provided on the job mentoring to providers and health education to patients on identification and management of side effects for hypertension medications as well as drug- drug interactions. In addition, the protocol emphasized adherence counseling and support for both HTN and HIV medicines.
-
2.
Routine HTN screening during each clinic visit
Clinic nurses trained PLHIV peer educators on BP measurement, which was performed using validated, automated Omron M6 BP machines [31]. Clinicians repeated the BP measurement for patients whose initial BP was > 140/90 mmHg. Though the clinic had already achieved optimal HTN screening, this was included in the implementation strategy to ensure continued attention to it by all providers.
-
3.
Task shifting of hypertension treatment
In addition to the aforementioned task shifting of screening practices, one doctor trained clinical officers and nurses on HTN medicine prescribing using the protocol in two-hour training sessions. These were followed by ongoing, one-on-one mentoring twice monthly to ensure protocol adherence and safe prescribing practices. We printed and provided a copy of the protocol to each clinician. In addition, two technical experts of the Department of NCDs at MoH provided quarterly support supervision on adherence to the protocol.
-
4.
Evidence-based HTN treatment protocol
We adapted HEARTS recommendations to develop our protocol which provided a simple, stepwise approach to the titration of amlodipine, valsartan, and hydrochlorothiazide as the first-, second-, and third-line therapies, respectively (Fig. 1) [13,14,15,16,17]. In addition to this stepwise approach, the protocol also included guidance for patients in higher risk groups.
-
5.
Consistent supply of HTN medicines free to patients
The choice of medicines was based on availability and local evidence of efficacy [32]. For the purpose of this study, we procured amlodipine, valsartan, and hydrochlorothiazide from a private not for-profit pharmaceutical access program [33, 34], endorsed and regulated by the Uganda MoH. The procurement cost to the study for these medicines ranged from 0.30USD to 1.50USD per patient per month and we provided them to patients at no cost. Outside the pharmaceutical access program, the cost of our protocol medicines in Uganda would have been approximately 10 times higher.
Fig. 1 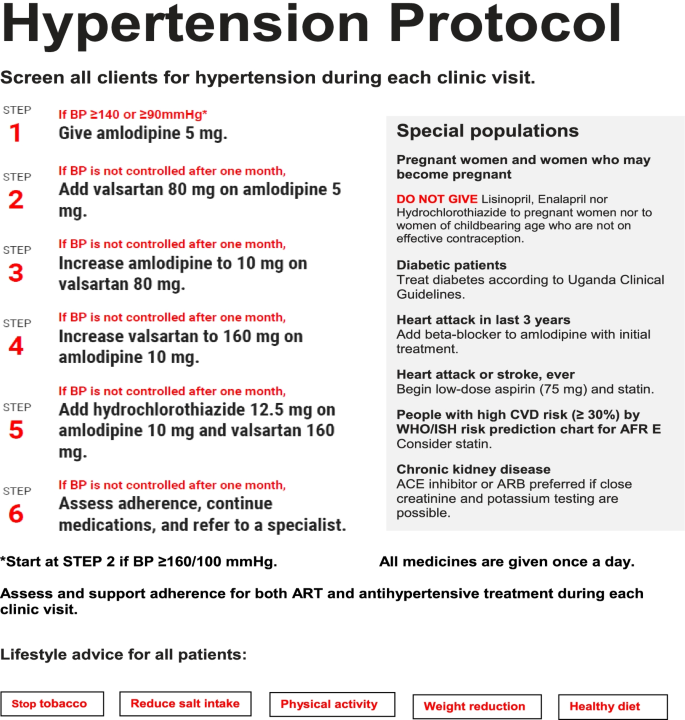
The hypertension management protocol at MJAP
-
6.
Inclusion of HTN-specific monitoring and evaluation tools
In our prior work, we had defined HTN monitoring indicators that parallel those used extensively in HIV care: Screening, Diagnosis, Initiation of treatment, Retention, Monitoring and Control [35]. Monitoring indicators are useful in evaluating the quality of health services and identifying gaps that should be targeted for continuous quality improvement [36]. In addition, we developed and shared quarterly targets on HTN care indicators with healthcare providers during bimonthly and quarterly performance review meetings. We adapted the HEARTS HTN register and CVD patient cards and distributed them to clinic providers. The CVD card was used to record the patent’s anthropometric measurements, comorbidities including diabetes, kidney disease, prior stroke and heart attack; blood pressure and blood sugar values; HTN medicines prescribed; ART regimen; laboratory findings including serums electrolytes, creatinine, urine protein, total cholesterol; and examination of the fundus and the foot. Each patient’s data was entered into both the CVD card and HTN register during each clinic visit.

Sampling of the study cohort
By August 1st, 2019, the clinic had 15,953 adult PLHIV aged ≥ 18 years. All these were screened for HTN and 3,892 (24.4%) were diagnosed with HTN. For the prospective cohort, we included all hypertensive PLHIV aged 18 years and above enrolled in HIV care at Mulago ISS who made at least one clinic visit between August 1st and September 30th, 2019. Study participants provided informed consent to be treated according to the adapted HEARTS protocol. Of the 3,892 hypertensive PLHIV, 1,015 patients accepted to be treated as per the treatment protocol and were enrolled into the study. The other 2,877 hypertensive PLHIV declined enrollment. For the 1,015 patients enrolled into integrated HTN/HIV treatment, we determined both HTN and HIV outcomes at baseline and followed them up for six months after introducing the adapted HEARTS implementation strategy. Of the 15 patients who were not retained at six months, six were lost to follow-up; five opted out due to side effects of HTN medications; three requested transfers to other HIV clinics and one died. At the end of six months, 1000 patients were retained in integrated HTN/HIV care (Fig. 2). We then compared HTN and HIV outcomes at baseline and six months after introducing the implementation strategy.

Flow chart of patient enrolment into integrated HTN/HIV Care
Data collection
We prospectively extracted data from the EMR. The EMR at Mulago ISS clinic was adopted from the Uganda MoH open medical records system, which managed patient data on HIV care [21]. The EMR was adapted to include blood pressure and anthropometric values and HTN medicines prescribed. We recorded data on indicators at every stage of the HTN and HIV care cascades. We developed the data collection tools to obtain information on the HTN and HIV care cascade at the Mulago ISS clinic and specifically mapped out the expected baseline and six-month outcomes at each cascade step according to national HIV guidelines and WHO recommendations [25, 26]. Throughout the study, we defined hypertension as “having a documented blood pressure (BP) ≥ 140/90 mmHg or documented use of HTN medications or documented history of hypertension” [35]. We described each cascade step as a proportion of the preceding step and reported them as follows for HTN and HIV: screened, diagnosed, treated, retained, monitored and controlled (Fig. 2). For all proportions, the denominator was the absolute number for each preceding cascade step. The primary outcome was HTN control (BP < 140/90 mmHg at the most recent clinic visit).
Data analysis
We described baseline characteristics using means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. We compared baseline characteristics of patients who were enrolled and those that were not enrolled into integrated HTN/HIV care.
We then compared the HTN and HIV outcomes at baseline and six months after introducing the implementation strategy in a cohort of hypertensive PLHIV who received integrated HTN/HIV care using a paired t-test statistic and paired sample proportions tests. We determined the six-month trend of the percentage of patients with controlled HTN from baseline to six months after introducing the implementation strategy. To determine proportions along the HTN and HIV care cascades, we conducted descriptive analyses and obtained frequencies and percentages of patients at each defined step compared with the preceding step.
We used a multivariate random effects logistic regression model to determine which baseline characteristics predicted HTN control at six months. We adjusted for age, sex, baseline BP, ART duration, baseline CD4 count, BMI, and baseline ART regimens. We analyzed the data using Stata (version 13). We followed the STROBE guideline in developing this manuscript [35].
Results
Baseline characteristics of study participants
Between August and September 2019, we enrolled a cohort of 1,015 hypertensive PLHIV into integrated HIV-hypertension with a mean age of 50.1 ± 9.5 years. Of these, 62.6% were female. Mean baseline systolic and diastolic BP were 154.3 ± 20.0 mmHg and 97.7 ± 13.1 mmHg respectively. A total of 270 (26.6%) participants were obese (body mass index > 30). Overall, the mean CD4 cell count before starting ART was 325.7 ± 251.7 cells per mm3. Both cohort participants and non-enrolled hypertensive patients had similar gender compositions. Cohort participants were older, had higher baseline BP, lower baseline CD4 counts, had been on ART longer and had higher BMIs compared to non-enrolled patients (Table 2).
Comparison of hypertension and HIV outcomes in the cohort at baseline (before introducing the HEARTS implementation strategy) and at six months of follow up
In this cohort, the mean systolic BP improved from 154.3 ± 20.0 mmHg at baseline to 132.3 ± 13.7 mmHg at six months (p < 0.001). Likewise, the mean diastolic BP improved from 97.7 ± 13.1 mmHg at baseline to 85.3 ± 9.5 mmHg at six months (p < 0.001). There was a significant improvement in HTN control from 9.3% at baseline to 74.1% at six months, (p < 0.001). HIV viral suppression remained high, 98.7% at baseline and 99.2% at six months (p = 0.712) (Table 3).
Additionally, there was a positive trend of hypertension control for six months after introducing the adapted HEART implementation strategy (Fig. 3).

Percentage of patients enrolled in integrated HTN/HIV care with controlled BP (N = 1015)
The denominator at each time point was 1015 patients who were enrolled into the cohort.
Baseline HIV Care
At baseline, all the 1,015 cohort participants had been tested for HIV, diagnosed and initiated on ART. All the 1,015 (100%) participants had been retained in care in the last six months and had viral load monitoring of whom 1,007 (99.2%) achieved HIV control (viral suppression) (Fig. 4A).

HTN and HIV care cascades at baseline (A) and six months (B)
The HTN and HIV care cascades in Fig. 4 above are for 1,015 hypertensive PLHIV who were enrolled in the cohort. The cascade at baseline was assessed through a retrospective study. Throughout the cascades, the denominator was the absolute number at each preceding step. Definitions of cascade steps: Screening = Number and % of patients who received an HIV test or whose blood pressure was measured before diagnosis; Diagnosis = number and % of patients who were diagnosed with HIV or HTN; Initiation = number and % of patients who were started on ART or HTN medications; Retention = number and % of patients who consistently received ART or HTN medications for six months: Monitoring = number and % of patients who had a viral load test or blood pressure measured while on HTN treatment and Control = number and % of patients with HIV viral suppression (viral load < 1000 copies/ml) or BP < 140/90 mmHg. The error bars indicate the 95% confidence intervals.
Baseline hypertension care
All the 1,015 cohort participants had been screened and diagnosed for HTN. Of these, 136 (13.4%) were initiated on HTN treatment and given only one agent, amlodipine. Of those initiated on HTN treatment, 22(16.2%) were retained and monitored for HTN. Only three (2.2% of those initiated on treatment) patients achieved HTN control (Fig. 4A). Expressed as a proportion of the total cohort, only 0.3% of patients were controlled.
HIV care cascade among PLHIV with HTN enrolled into the cohort at six months
All 1,015 PLHIV with HTN who were enrolled into integrated HTN/HIV care had been initiated on ART and HTN medicines, of whom 1,011 (99.6%) were retained in HIV care at six months and had a timely viral load test, with 1,002 (99.1%) achieving HIV control (viral suppression) (Fig. 4B). Expressed as a proportion of the total cohort, 98.7% of enrolled patients had HIV viral suppression at six months.
HTN care cascade among PLHIV with HTN at six months
All 1,015 (100%) cohort participants were initiated on HTN treatment and 1,000 (98.5%) were retained in HTN care at six months. All those retained were monitored for HTN at six months and 752 (75.2%) achieved HTN control (Fig. 4B). Expressed as a proportion of total cohort, 74.1% of enrolled patients achieved a blood pressure of < 140/90 at six months. Of the patients with controlled HTN at six months, 151 (20%) were on one protocol medicine (amlodipine 5 mg), 587 (78%) were on more than one protocol medicine, and 12 (2%) were on non-protocol hypertension medicines (Table 4).
Independent predictors of HTN control at six months of treatment
Out of numerous physical, demographic, and clinical characteristics examined, the only independent predictors of HTN control at six months were being on ART for longer than two years. These individuals were two to four times more likely than those with shorter ART durations to achieve HTN control at six months. The likelihood of hypertension control increased with ART duration. Additionally, individuals who had a suppressed HIV viral load were 3.2 times more likely to achieve HTN control compared to those with a non-suppressed viral load (Table 5).
Discussion
In this study, we aimed to use the BCW framework to adapt a WHO HEARTS-based implementation strategy to integrate HTN management into HIV care through stakeholder engagement and local contextualization. Using this strategy, our HTN control among PLHIV and HTN increased from 9% at baseline to 74% at six months. The HEARTS technical packages for CVD control were introduced to improve HTN control in multiple settings [13,14,15,16,17]. However, to our knowledge, this is the first study to adapt the WHO HEARTS technical packages to integrate HTN management into a clinical setting for HIV care.
Among the HEARTS components, we believe that successful HTN/HIV integration in our setting was and will be hinged on the following: a simple, stepwise HTN protocol [13], consistent access to HTN medicines [15], task shifting of HTN screening and treatment to lower cadres of healthcare providers [17], strengthening HTN monitoring and evaluation and training and mentoring of healthcare providers [37, 38].
Our implementation strategy was effective in improving HTN control at this large urban HIV clinic. At baseline, the clinic had very nearly met or exceeded all three UNAIDS 90–90-90 goals regarding ART initiation, retention in care and viral suppression. In addition, the clinic had already achieved universal BP screening for all adult PLHIV, demonstrating a high prevalence of HTN (24.3%) [21, 22]. Despite a high prevalence of HTN, initiation of HTN treatment, retention, and HTN control were suboptimal (Fig. 4A). Similarly stark findings have been identified in other parts of SSA and in our previous studies in rural Uganda [21, 39]. Of the 3,892 hypertensive PLHIV at the clinic, we enrolled 1,015 patients into integrated HTN/HIV care. The remaining 2,877 patients declined enrollment. The major reason for non-enrollment was patients who were already taking other anti-hypertensive medications either from other health facilities or bought from retail pharmacies. At six months after implementing the integrated HTN/HIV care, our program had all the 1,015 enrolled hypertensive PLHIV receiving integrated HTN/HIV care. In line with the WHO and MoH HIV test and treat policy [25, 26], all enrolled PLHIV with HTN were initiated or maintained on ART and HTN medicines. Among the patients in our cohort, retention in HIV care, viral load monitoring and HIV control were all sustained above 95% both at baseline and six months (Fig. 4). These findings suggest that integrated HTN/HIV care sustains an optimal HIV care cascade.
The integrated HTN/HIV program initiated all hypertensive PLHIV in the cohort to HTN treatment, retained almost all of them in care, and routinely monitored most during each clinic visit. Importantly, HTN control at six months, a HEARTS Core Indicator, reached 74% [18]. Similarly high levels of HTN control were registered in the Kaiser Permanente HTN program of North California, which utilized a stepwise HTN protocol that had a thiazide diuretic as first line medication [40, 41]. This level of HTN control among PLHIV and the general population has not been achieved in SSA [21, 39]. In Uganda, a community-based epidemiologic study found a HTN control rate of 2.2% [42]. Our cohort participants were older and had been on ART longer than non-enrolled patients. These factors may have contributed to better adherence to both ART and HTN medications and hence better HTN control.
In our study, the rate of attrition from HTN care was low at 1.5%. In addition, there were few side effects of BP medications prescribed in our study, further supporting the safety and feasibility of our approach.
The medicines on our protocol, which we procured from a pharmaceutical access program, were available to the private not for profit sector and not yet adopted by the public health facilities. Further scale up of these low priced and effective agents will require including them into the essential medicines list of Uganda so that patients in the public health facilities can benefit. Our protocol has been adopted by the Uganda MoH and integrated into guidelines to integrate hypertension management into HIV care for national scale up.
Finally, patients who had been on ART for more than two years were more likely to achieve HTN control than those with shorter ART durations. Similar findings have been replicated in HIV programs across SSA regarding HIV and HTN control [43,44,45,46,47]. In this patient population, adherence to HIV medication is likely to predict adherence to antihypertensives. This was further emphasized by the better HTN control among patients who had achieved a suppressed HIV viral load which resulted from high levels of ART adherence. Additionally, the effect of a long duration of ART may be partly confounded by age [47,48,49].
Limitations
Due to supply chain limitations, hydrochlorothiazide was not supplied until after the six-month follow up. Long-term follow up of our cohort will determine the added effectiveness of hydrochlorothiazide. We used a pre-post study design and described a six-month trend of hypertension control in our cohort after introducing the implementation strategy. This minimized the influence of autocorrelation in the follow up period. However, we did not analyze the pre-intervention trend because we did not collect that data. Therefore, baseline results may be affected by autocorrelation and seasonality. In this study, we did not conduct random sampling of cohort participants. The convenience sampling renders findings of this study less generalizable among diverse populations. Additionally, the pre-intervention assessment of BP could have sensitized patients to seek better care for HTN. This could confound the achievement and predictors of HTN control at six months. We were unable to control for unmeasured confounders since the study lacked a control group. Despite these limitations, the outcomes reported provide preliminary evidence for the effectiveness of an adapted HEARTS intervention on HTN control among PLHIV.
Conclusions
An adapted WHO HEARTS-based implementation strategy at a large, urban HIV center facilitates integration of HTN and HIV care and improves HTN outcomes while sustaining HIV control. Further implementation research of the HEARTS strategy is needed to study HTN/HIV integration in varied clinical settings among diverse populations.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COM-B:
-
Capability, Opportunity, Motivation and Behavior
- HTN:
-
Hypertension
- PLHIV:
-
Persons Living with HIV
- CVD:
-
Cardiovascular Disease
- NCD:
-
Non-Communicable Disease
- ART:
-
Antiretroviral Therapy
- WHO:
-
World Health Organization
- MoH:
-
Ministry of Health
References
Pangmekeh PJ, Awolu MM, Gustave S, Gladys T, Cumber SNJTPAMJ. Association between highly active antiretroviral therapy (HAART) and hypertension in persons living with HIV/AIDS at the Bamenda regional hospital, Cameroon. Pan Afr Med J. 2019;33:87.
Coetzee L, Bogler L, De Neve JW, Bärnighausen T, Geldsetzer P, Vollmer SJJotIAS. HIV, antiretroviral therapy and non‐communicable diseases in sub‐Saharan Africa: empirical evidence from 44 countries over the period 2000 to 2016. J Int AIDS Soc. 2019;22(7):e25364.
Osetinsky B, Hontelez JAC, Lurie MN, McGarvey ST, Bloomfield GS, Pastakia SD, et al. Epidemiological and health systems implications of evolving HIV and hypertension in South Africa and Kenya. Health Aff (Millwood). 2019;38(7):1173–81.
Kwarisiima D, Atukunda M, Owaraganise A, Chamie G, Clark T, Kabami J, et al. Hypertension control in integrated HIV and chronic disease clinics in Uganda in the SEARCH study. BMC Public Health. 2019;19(1):511.
Mutemwa M, Peer N, de Villiers A, Mukasa B, Matsha TE, Mills EJ, et al. Prevalence, detection, treatment, and control of hypertension in human immunodeficiency virus (HIV)-infected patients attending HIV clinics in the Western Cape Province, South Africa. Medicine (Baltimore). 2018;97(35):e12121.
Walsh KF, Hee Lee M, Martelly S, Pierre MM, Joseph J, Gustin M, et al. Integrating hypertension services at an HIV clinic in Port‐au‐Prince, Haiti: a report from the field. J Clin Hypertens (Greenwich). 2018;20(10):1485–92.
Gimbel S, Mocumbi AO, Ásbjörnsdóttir K. Systems analysis and improvement approach to optimize the hypertension diagnosis and case cascade for PLHIV individuals (SAIA-HTN): a hybrid type III cluster randomized trial. Implement Sci. 2020;15(1):15.
Dowdy DW, Powers KA, Hallett TB. Towards evidence-based integration of services for HIV, non-communicable diseases and substance use: insights from modelling. J Int AIDS Soc. 2020;23(Suppl 1):e25525.
Garrib A, Birungi J, Lesikari S, Namakoola I, Njim T, Cuevas L, et al. Integrated care for human immunodeficiency virus, diabetes and hypertension in Africa. Trans R Soc Trop Med Hyg. 2019;113(12):809–12.
Althoff KN, Gebo KA, Moore RD, Boyd CM, Justice AC, Wong C, et al. Contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the USA and Canada: a collaboration of cohort studies. The lancet HIV. 2019;6(2):e93–104.
Mensah GA. Epidemiology of stroke and high blood pressure in Africa. Heart. 2008;94(6):697–705.
Van Hout M, Bachmann M, Lazarus JV, Shayo EH, Bukenya D, Picchio CA, et al. Strengthening integration of chronic care in Africa: protocol for the qualitative process evaluation of integrated HIV, diabetes and hypertension care in a cluster randomised controlled trial in Tanzania and Uganda. BMJ open. 2020;10(10):e039237.
HEARTS Technical package for cardiovascular disease management in primary health care: evidence-based treatment protocols. Geneva: World Health Organization; 2018.
HEARTS Technical package for cardiovascular disease management in primary health care: healthy-lifestyle counselling; Geneva: World Health Organization; 2018.
HEARTS Technical package for cardiovascular disease management in primary health care: access to essential medicines and technology. Geneva: World Health Organization; 2018.
HEARTS technical package for cardiovascular disease management in primary health care: risk based CVD management. Geneva: World Health Organization; 2020.
HEARTS Technical package for cardiovascular disease management in primary health care: team-based care. Geneva: World Health Organization; 2018.
HEARTS Technical package for cardiovascular disease management in primary health care: systems for monitoring. Geneva: World Health Organization; 2018.
Webster R, Murphy A, Bygrave H, Ansbro É, Grobbee DE, Perel P. Implementing Fixed Dose Combination Medications for the Prevention and Control of Cardiovascular Diseases. Global Heart. 2020;15(1):57.
Kaur P, Kunwar A, Sharma M, Mitra J, Das C, Swasticharan L, et al. India Hypertension Control Initiative-Hypertension treatment and blood pressure control in a cohort in 24 sentinel site clinics, India. J Clin Hypertens (Greenwich). 2020;23(4):720–9. https://doi.org/10.1111/jch.14141.
Muddu M, Ssinabulya I, Kigozi SP, Ssennyonjo R, Ayebare FX, Katwesigye R, et al. Hypertension care cascade at a large urban HIV clinic in Uganda: a mixed methods study using the Capability, Opportunity, Motivation for Behavior Change (COM-B) model. Implement Sci Commun. 2021;2(1):121.
An ambitious treatment target to help end the AIDS epidemic. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90–90–90. Geneva: 2017. http://www.unaids.org/en/resources/documents/2017/90-90-90. Accessed 29 Oct 2020.
Michie S, Van Stralen MM, West RJIS. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Barker F, Atkins L, de Lusignan S. Applying the COM-B behaviour model and behaviour change wheel to develop an intervention to improve hearing-aid use in adult auditory rehabilitation. Int J Audiol. 2016;55(sup3):S90–8.
March 2014 supplement to the 2013 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. Geneva: World Health Organization; 2014.
Consolidated guidelines for prevention and treatment of HIV in Uganda. Kampala: Uganda Ministry of Health; 2018. p. 74–5.
McMillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm. 2016;38(3):655–62.
Crayton E, Wright AJ, Ashworth M. Improving medication adherence in stroke survivors: the intervention development process. BMC Health Serv Res. 2018;18(1):772.
Smits S, McCutchan G, Wood F, Edwards A, Lewis I, Robling M, et al. Development of a behavior change intervention to encourage timely cancer symptom presentation among people living in deprived communities using the behavior change wheel. Ann Behav Med. 2018;52(6):474–88.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
Topouchian JA, El Assaad MA, Orobinskaia LV, El Feghali RN, Asmar RG. Validation of two automatic devices for self-measurement of blood pressure according to the International Protocol of the European Society of Hypertension: the Omron M6 (HEM-7001-E) and the Omron R7 (HEM 637-IT). Blood Press Monit. 2006;11(3):165–71.
Ojji DB, Poulter N, Damasceno A, Sliwa K, Smythe W, Kramer N, et al. Rationale and design of the comparison of 3 combination therapies in lowering blood pressure in black Africans (CREOLE study): 2× 3 factorial randomized single-blind multicenter trial. Am Heart J. 2018;202:5–12.
Manji I, Pastakia SD. Novartis Access: a small step towards increased access for non-communicable disease care. Lancet Glob Health. 2019;7(4):e398–9.
Rockers PC, Laing RO, Ashigbie PG, Onyango MA, Mukiira CK, Wirtz VJ. Effect of Novartis Access on availability and price of non-communicable disease medicines in Kenya: a cluster-randomised controlled trial. Lancet Glob Health. 2019;7(4):e492–502.
Muddu M, Tusubira AK, Sharma SK, Akiteng AR, Ssinabulya I, Schwartz JI. Integrated hypertension and HIV care cascades in an HIV treatment program in eastern Uganda: a retrospective cohort study. JAIDS J Acquir Immune Defic Syndr. 2019;81(5):552–61.
Subbaraman R, Nathavitharana RR, Satyanarayana S, Pai M, Thomas BE, Chadha VK, et al. The tuberculosis cascade of care in India’s public sector: a systematic review and meta-analysis. PLoS Med. 2016;13(10):e1002149.
Musinguzi G, Bastiaens H, Wanyenze RK, Mukose A, Nuwaha F. Capacity of health facilities to manage hypertension in Mukono and Buikwe districts in Uganda: Challenges and recommendations. PLoS ONE. 2015;10(11):e0142312.
Chang H, Hawley NL, Kalyesubula R, Siddharthan T, Checkley W, Knauf F, et al. Challenges to hypertension and diabetes management in rural Uganda: a qualitative study with patients, village health team members, and health care professionals. Int J Equity Health. 2019;18(1):38.
Muddu M, Tusubira AK, Nakirya B, Nalwoga R, Semitala FC, Akiteng AR, et al. Exploring barriers and facilitators to integrated hypertension-HIV management in Ugandan HIV clinics using the Consolidated Framework for Implementation Research (CFIR). Implement Sci Commun. 2020;1(1):1–14.
Jaffe MG, Young JD. The Kaiser Permanente Northern California story: improving hypertension control from 44% to 90% in 13 years (2000 to 2013). The Journal of Clinical Hypertension. 2016;18(4):260–1.
Fontil V, Gupta R, Moise N, Chen E, Guzman D, McCulloch CE, et al. Adapting and evaluating a health system intervention from Kaiser Permanente to improve hypertension management and control in a large network of safety-net clinics. Circ: Cardiovasc Qual Outcomes. 2018;11(7):e004386.
Geldsetzer P, Manne-Goehler J, Marcus ME, Ebert C, Zhumadilov Z, Wesseh CS, et al. The state of hypertension care in 44 low-income and middle-income countries: a cross-sectional study of nationally representative individual-level data from 1·1 million adults. Lancet. 2019;394(10199):652–62.
Brennan AT, Jamieson L, Crowther NJ, Fox MP, George JA, Berry KM, et al. Prevalence, incidence, predictors, treatment, and control of hypertension among HIV-positive adults on antiretroviral treatment in public sector treatment programs in South Africa. PLoS One. 2018;13(10):e0204020.
Benzekri NA, Seydi M, Doye IN. Increasing prevalence of hypertension among HIV-positive and negative adults in Senegal, West Africa, 1994–2015. PLoS ONE. 2018;13(12):e0208635.
Mathebula RL, Maimela E, Ntuli NS. The prevalence of selected non-communicable disease risk factors among HIV patients on anti-retroviral therapy in Bushbuckridge sub-district, Mpumalanga province. BMC Public Health. 2020;20(1):247.
Fiseha T, Belete AG, Dereje H, Dires A. Hypertension in HIV-Infected Patients Receiving Antiretroviral Therapy in Northeast Ethiopia. Int J Hypertens. 2019;2019:4103604.
Divala OH, Amberbir A, Ismail Z, Beyene T, Garone D, Pfaff C, et al. The burden of hypertension, diabetes mellitus, and cardiovascular risk factors among adult Malawians in HIV care: consequences for integrated services. BMC Public Health. 2016;16(1):1243.
Haldane V, Legido-Quigley H, Chuah FLH, Sigfrid L, Murphy G, Ong SE, et al. Integrating cardiovascular diseases, hypertension, and diabetes with HIV services: a systematic review. AIDS Care. 2018;30(1):103–15.
Magafu MG, Moji K, Igumbor EU, Magafu NS, Mwandri M, Mwita JC, et al. Non-communicable diseases in antiretroviral therapy recipients in Kagera Tanzania: a cross-sectional study. Pan Afr Med J. 2013;16:84.
Acknowledgements
We are grateful to the following persons for their invaluable support: The clinic manager and staff of Mulago ISS clinic, and all the research assistants who participated in this study. We appreciate the guidance of Professor Moses R. Kamya.
Funding
Research reported in this manuscript was supported by Resolve to Save Lives under Award Number MJAP/VITAL 2019/001 and the Fogarty International Centre of the National Institutes of Health, D43 TW010037 and K43TW011963-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of Resolve to Save Lives or the National Institutes of Health. The funders had no role in the study design, data collection, analysis or interpretation. MM and JIS had full access to all the data and had the final responsibility for the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
MM, FCS, IS, ARK, SPK, JIS and IK were responsible for the design of the study and interpretation of data. MMB, CN, IK, RS, FA, RK and MM led data collection and interpretation. CN, SPK, MM and MMB performed data analysis. FM, GM and CTL participated in the interpretation of data. All authors participated in writing the initial draft of the manuscript. MM and JIS participated in writing the final manuscript. All authors read and approved the final manuscript before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided verbal informed consent to participate in the study since they received integrated hypertension and HIV treatment as part of routine clinical care based on the WHO HEARTS guidelines. Additionally, the medications on our hypertension management protocol were already registered by the National Drug Authority for use in Uganda. The study protocol was approved by The AIDS Support Organization (TASO) Institutional Review Board (IRB) number TASOREC/040/19-UG-REC-009 and the Uganda National Council for Science and Technology (UNCST) number HS 2644.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no relevant competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Muddu, M., Semitala, F.C., Kimera, I. et al. Improved hypertension control at six months using an adapted WHO HEARTS-based implementation strategy at a large urban HIV clinic in Uganda. BMC Health Serv Res 22, 699 (2022). https://doi.org/10.1186/s12913-022-08045-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08045-8